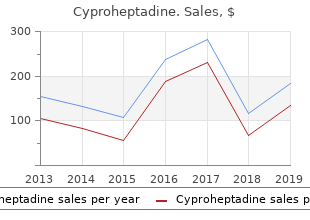
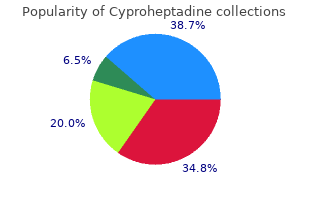
Cyproheptadine
"4mg cyproheptadine, allergy symptoms of gluten intolerance".
By: C. Mirzo, M.A., M.D.
Co-Director, Idaho College of Osteopathic Medicine
The crack noise or joint cavitation is the result of generation or collapse of a gaseous bubble in the synovial fluid allergy treatment by baba ramdev quality cyproheptadine 4mg. Cineradiographic studies reported increased joint space and carbon dioxide gas production/ breakdown after thrust manipulation allergy testing uk boots buy cyproheptadine overnight. Because carbon dioxide is the gas with the higher miscibility within the synovial fluid allergy honey buy cyproheptadine 4mg line, this increase in carbon dioxide levels has been suggested as the mechanism to increase range of motion in the joint after manipulation. It has also been hypothesized that the cavitation would initiate certain reflex relaxation of the periarticular musculature. After the manipulation, the joint takes approximately 15 minutes to rearrange the gas particles and allow another cavitation sound. Some people believe that if there is no noise, nothing has happened; this belief is incorrect. Different grading systems exist for joint mobilization: (1) grading for traction mobilization technique; (2) grading for sustained joint-play technique; (3) grading for oscillatory technique. The most widespread system used is the grading system for oscillatory technique proposed by Maitland, which has five grades of movement. Grade 2—slow, large-amplitude movements that do not reach the resistance or limit of the range. Grade 5—fast, small-amplitude, high-velocity movements (thrust) performed beyond the pathologic limitation of the range Manual Therapy 105 Grades 1 through 4 are used for mobilization techniques and generally use oscillatory movements. Grade 5 is used for the thrust technique and is indicated when resistance limits movement, in the absence of pain in that direction. Is there evidence that manual therapy is effective in the treatment of spinal conditions? In fact there is a growing body of evidence of the effectiveness of manual therapy for several spinal conditions. Therefore, to date it seems that joint techniques are more effective than muscle or soft tissue techniques. Among the joint techniques for individuals with acute low back pain, there is moderate evidence that manipulation provides more short-term pain relief than mobilization. This study reported that although all groups improved over time, manipulation followed by exercise achieved the most significant benefits, followed by the spinal manipulation group and lastly by the exercise group. Other more recent studies have validated the idea that a high probability of success from spinal manipulation depends on the importance of matching individual patients with the correct intervention. These studies developed a clinical prediction rule that demonstrated that clinicians can accurately identify patients with low back pain who are likely to benefit (achieve at least 50% improvement in disability) from spinal manipulation. The five predictors of success were short symptom duration, low treatment apprehension levels, lumbar hypomobility, adequate hip internal rotation range of motion, and no symptoms distal to the knee. The probability of a successful outcome among patients who met at least four of the five criteria in the rule increased from 45% to 95%. In essence, the combination of both manual therapy with exercises and the appropriate patient intervention selection to apply the techniques seems to increase the beneficial effects of manual therapy techniques. A recent systematic reviewreported that spinal manipulation and/or mobilization is superior to general practitioner management for short-term pain reduction in patients with chronic neck pain. There is moderate evidence that mobilization is superior to physical therapy and family physician care. There is no evidence to support the use of manipulation versus mobilization for patients with neck pain. It is theorized that biomechanical relationships between the cervical spine and thoracic spine make it possible that disturbances in joint mobility in the thoracic spine may 106 Special Topics contribute to movement restrictions and pain in the cervical region. There is also limited evidence that the combination of thoracic spine manipulation and intermittent cervical traction for patients with cervical compressive myelopathy attributes to herniated disk and that patients with cervical radiculopathy show decreased pain and improved function. Is there evidence that manual therapy is effective in treating cervicogenic headache? Systematic reviews suggest that mobilization/manipulation is effective for patients with cervicogenic headache.
All investigators are required to allergy forecast birmingham al cheap cyproheptadine 4mg with visa conduct themselves at all times in accordance with Good Clinical Practices allergy forecast oakville buy discount cyproheptadine 4mg. Investigators are expected to allergy vinegar symptoms buy cheap cyproheptadine 4 mg on line commit themselves to ethical and professional conduct of clinical research. Commitment to preserving the physician’s, medical community, and public’s trust is ensured by conducting research at the highest scientific and ethical standards. The planned sample size will also provide high confidence in ruling out rare adverse events. For more common outcomes, the statistical power for specific relative risk estimate is greater. For example, with 2,000 patients in each group there would be 90% power to detect a difference between two approaches for which the incidence rates of events were 3% and 5%. There will be several major advantages of the registry design as opposed to a system of spontaneous reporting. In contrast, systems that rely on spontaneous reporting have incomplete numerator data and lack denominator data. The ability to calculate incidence rates greatly facilitates both descriptive epidemiology and signal detection. Thus, descriptive statistics with 95% confidence intervals will be determined for the safety and effectiveness outcomes to provide precise estimates of incidences. To assure the feasibility of this approach, we have conducted a preliminary analysis of these data to identify the number of patients who will be included in the control cohort. The sample size should be sufficient to address questions on relatively rare outcomes. For example, at age 68 years (the median age in our control cohort), the probability of death in the next 12 months is 1. Comparative effectiveness studies rely on the ability to adequately account for differences between the treatment groups. Such data will support standard statistical methods including logistic, Cox, and other regression methods, and the development of propensity scores and risk scores for risk adjustment. There is a theoretical risk of breach of confidentiality or a data security loss although exhaustive efforts will be made to minimize this inherent risk. All sites must demonstrate proper physical and electronic security measures in order to participate in the registry. Securing in a separate location and limiting access to information linking codes assigned to the registry information with direct participant identifiers 3. All computers will be used to collect and send data during implementation of the study or to receive or store data at the central location will be password protected. A password will be required to open Windows and a second, different password will be required to open the electronic data capture system, Viedoc™. Electronic forms will be stored on a secure dedicated server with appropriate firewalls. This technology is the same as that used for online e commerce applications to protect consumer information such as name, address, and credit card details. Servers are scanned for viruses and systems are in place to detect attempts at unauthorized entry. All transactions to the database are stored in archive logs as re-do data and are accessible to enable quick recovery of all data should the need arise. For example, patients can receive an automatic text message or email that opens to a follow-up electronic questionnaire for long-term follow-up. Interested investigators will be asked to submit a brief application including their research question(s) and requested criteria and variables. The Data Access and Publication Committee will review these requests to solely ensure that the request is appropriate and within the scope of the registry. Each site will need to provide documentation of receiving and passing a training course in human subject’s protections. Approval of both the protocol and the consent form must be obtained before any participant is enrolled. Extensive discussion of risks and possible benefits of study participation will be provided to participants and their families, if applicable. A consent form describing in detail the study procedures and risks will be given to the participant.
Buy 4mg cyproheptadine amex. Food Allergies : Signs Symptoms And Treatment For Food Allergy.
Lateral epicondylitis in a professional tennis player with a history of chronic right lateral elbow pain allergy testing loveland co purchase generic cyproheptadine. The torn deep fibers (arrowheads) are retracted just distal to allergy symptoms list purchase genuine cyproheptadine on line the hypoechoic area allergy forecast grand rapids mi purchase 4mg cyproheptadine otc. Note the integrity of the underlying lateral ulnar collateral ligament (asterisks). An isolated liga Supinator Syndrome ment tear appears as discontinuity of the deep (Posterior Interosseous Neuropathy) est fibers of the extensor tendon origin, whereas tears involving both the ligament and the common Supinator syndrome, also referred to as “posterior extensor tendon cause a full-thickness interrup interosseous syndrome” or “radial tunnel syndrome”, tion of fibers over the lateral aspect of the radio is a rare compression neuropathy of the upper limb capitellar joint and soft tissue hematoma around affecting the posterior interosseous nerve just near the proximal margin of the capitellum (Connell or behind the supinator muscle (Spinner 1968). Dynamic scanning during careful nerve is vulnerable to injury at the proximal edge varus stressing can disclose lateral ulnar collateral of the superficial belly of the supinator muscle that ligament injury by depicting widening of the lat forms a free, strong, fibrous arch, the “arcade of eral elbow joint space compared with the opposite Frohse”. Complete tear of the common extensor tendon and the lateral ulnar collateral ligament. Martinoli fan-shaped recurrent radial vessels or by tightness thickened and thinned segments between the super of the passage within the superficial and deep layers ficial and deep bellies of the supinator muscle as a of the supinator. In addi by a variety of soft-tissue masses, such as paraosteal tion, the nerve may be seen encased by hypoechoic lipomas and deep ganglia. Clinically, the posterior interos seous neuropathy produces a clinical picture dis tinct from a lesion of the radial nerve in the arm. Extension of the fingers at the Distal Triceps Tendon Tear metacarpophalangeal joints is impaired and there is deficit of abduction and extension of the thumb. Distal triceps tendon tear is an uncommon condi In addition, posterior interosseous neuropathy may tion that mostly occurs at or close to the olecranon cause burning pain and tenderness over the lateral process of the ulna, often associated with a fleck elbow, possibly mimicking a “resistant lateral epi of bone attached to the retracted tendon as a result condylitis”. The compressed nerve typically appears outstretched arm, or relates to a direct blow onto swollen and hypoechoic proximal to or inside the the olecranon process. In post-trau the olecranon bursa, anabolic steroid abuse and matic settings, the nerve may appear displaced by pre-existing tendinosis may also have a role in the a malaligned radial head and may exhibit alternate tendon rupture. Posterior interosseous nerve syndrome in a young woman who presented with a intense weakness in extending the right fingers, especially involving thumb movements, and b a longitudinal skin depression (arrow) over the dorsum of the forearm following a contusion to the lateral elbow. This latter nerve is irregularly swollen as it passes over the bone b (large arrows) as a result of the scar encasement visible in a 386 S. Complete rupture of the distal triceps tendon presents clinically with complete inability to Olecranon bursitis, the most common superficial extend the elbow, given the absence of other muscles bursitis in the body, appears clinically as a lump that can assist in this movement. In the acute phase, overlying the olecranon process due to fluid dis however, the clinical diagnosis may be hampered by tension or hypertrophy of the synovial membrane. Calcific enthesopathy of the distal that require immediate surgery to avoid retraction triceps tendon is a predisposing factor. However, of the tendon and partial tears that may be treated bursal distension can be appreciated in a variety conservatively. Staphylococcus, tuberculosis); also patients delineate the degree of tendon retraction and can under chronic hemodialysis treatment may occa help in the diagnosis of atypical ruptures, such as in sionally have olecranon bursitis. When bursitis is cases of tears occurring at the myotendinous junc secondary to infection or gout, bursal swelling is tion (Fig. Due to the close anatomic relation of typically painful and associated with skin warmth the distal triceps tendon with the medial epicondyle and erythema due to local inflammatory changes. Similarly, when the patient tive tendinosis can be appreciated as a thickened has a history of tuberculous disease, a specific etiol hypoechoic tendon. Chronic traumatic olecranon bursitis in a manual laborer who had recently injured several times his posterior right elbow. In this case, needle aspiration of the bursal b c fluid revealed calcium milk solution following bursal rupture. In such patients, subcuta to the olecranon bursa, an additional small subolec neous nodules can be seen in the olecranon region ranon bursa can exist at the posterior aspect of the and along the proximal ulna. In rare instances, this bursa be considered in the differential diagnosis as they can can be involved by the same processes affecting the mimic olecranon bursitis or a solid neoplasm Distal larger olecranon one (Fig. The olecranon bursa (arrowheads) shows irregular wall thickening and ill-defined margins due to coexisting peribursal cellulitis.
All four networks were evaluated; however allergy symptoms cats generic 4mg cyproheptadine otc, the lack of evidence available to allergy shots under the tongue purchase cyproheptadine now inform networks 2 allergy treatment brunswick ga buy cheap cyproheptadine 4mg, 3 and 4 led to a lack of stability in the models, particularly a lack of stability in between-study variance. For completeness these analyses have been presented in Appendix 10 although no conclusions can be drawn from the results presented. Only the results for the network of any intervention and of any quality (network 1) are presented here. The slightly higher number of trials included in this network allows the model to achieve stability. Network 1: studies of any intervention and of any quality Tere were nine trials with data that could be used in the analysis of pain at or close to 3 months. Tese nine trials formed a connected network of nine interventions compared with placebo. For example, there were two studies available for the comparison of steroid with placebo. Where there is no line there were no studies available, for example physical therapy without mobilisation versus arthrographic distension and steroid. The models were run for 100,000 iterations and were not sensitive to the length of burn-in. Stable estimates of treatment efect, CrIs and between-study heterogeneity were produced by the models using a uniform prior of (0, 5), (0, 10) and (0, 15). Convergence, determined by graphical traces and the Brooks–Gelman–Rubin statistic, was achieved. The model was a good ft as the residual deviance was close to the number of data points. Table 56 presents the treatment efects compared with placebo in order of mean efectiveness. Steroid combined with physiotherapy showed a benefcial treatment efect compared with placebo with 95% CrIs that did not cross the line of no efect. The 95% CrI of the treatment efect of physical therapy without mobilisation and physiotherapy combined with placebo marginally crossed the line of no efect. Tere was no clear diference between the interventions in treatment efects, that is, the CrIs overlapped. Steroid combined with physiotherapy showed a clinically signifcant as well as statistically signifcant reduction in pain, with a 95% CrI that corresponded to a clinically signifcant reduction in pain only: –28. Opportunities for comparison with standard meta-analysis are limited as most of the studies were not pooled in a quantitative synthesis. It was possible to compare with the standard meta analyses for steroid plus physiotherapy versus placebo and steroid versus placebo. Homogeneity The assumption of homogeneity is that trials are sufciently homogeneous to be quantitatively combined. In the analysis presented, placebo included sham distension, saline injections and placebo laser. Although we believed that it was appropriate to pool diferent types of placebo, it could be argued that these are not similar enough because of the difering degree of invasiveness. This would suggest that the populations of the invasive studies had a longer duration and possibly more treatment-resistant forms of frozen shoulder than those in the conservative treatment studies. However, this assumption requires that the treatments involved belong to closed loops in the network of evidence, such as that seen in a connected polygonal structure. Methodological similarity Of the nine studies included in the analysis, fve were of at least satisfactory quality (method of randomisation was adequate and outcome assessment was blinded)16,35,39,41,43 and four were not. However, this model was unstable and, although presented in Appendix 10, the reliability of the data included in the analysis presented is uncertain and does not allow a robust assessment of the impact of quality. Summary Nine interventions formed part of a connected network with placebo and the evidence was informed by all nine trials. The remaining treatments had 95% CrIs that crossed the line of no efect and which contained clinically insignifcant values. Overall, there was no clear diference in the treatment efects of any of the interventions, that is, the CrIs overlapped.