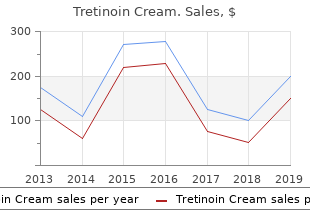
Tretinoin Cream
"Purchase tretinoin cream with paypal, acne jawline".
By: D. Joey, M.A., M.D., M.P.H.
Medical Instructor, Louisiana State University School of Medicine in Shreveport
The mucus is produced by mucous (goblet) cells in the surface respiratory epithelium and subepithelial glands in the lamina propria acne help order tretinoin cream visa. The synchronized beating of surface cilia propels the mucus and entrapped particulates from the main nasal chamber caudally to acne under arms buy discount tretinoin cream line the nasopharyngeal meatus acne treatments that work discount tretinoin cream online american express. The auditory tubes also enter the nasal airway in the dorsolateral aspect of the nasopharynx. The auditory tubes are also lined with ciliated respiratory epithelium, which under normal circumstances, allows equilibration of middle ear pressure with airway pressure, and propels accumulated middle ear secretions into the nasopharynx. Since this site is one of the first lines of defense against inhaled pathogens, dusts, and irritant gases, compromises in mucociliary clearance could lead to increased nasal infections and increased susceptibility to lower respiratory tract diseases. From this site, nasopharyngeal contents are cleared to the oropharynx, where they can be swallowed into the esophagus and cleared through the digestive tract or expectorated. Olfactory Function the ethmoturbinates lining the dorsal and caudal main chamber of the nasal cavity are lined by olfactory epithelium, a sensory neuroepithelium that is responsible for olfactory function. This epithelium contains bi-polar neurons that pass through the cribriform plate and synapse directly in the olfactory bulb of the brain. Once the condition has been localized as precisely as possible, specialized diagnostic procedures can be employed to obtain a diagnosis. When time and resources permit, staging the diagnostic process to rule out differential diagnoses can provide a more complete assessment and facilitate better therapeutic recommendations. Because many cases of nasal disease are eventually treated empirically or symptomatically, ruling out the conditions that will not respond to routine empirical therapeutic options should occur as early as possible. These include non-respiratory causes of nasal symptoms (alimentary, regurgitation and reflux, tooth root abscesses, hypertension, coagulopathies), and structural obstructive abnormalities (choanal atresia, choanal strictures, nasopharyngeal polyps, nasopharyngeal stenosis, caudal aberrant turbinates, nasal foreign bodies). Neoplastic causes are also important to rule out as early as possible, as these may be life-threatening or time-sensitive. Clients may be more inclined to treat nasal tumors if they�re diagnosed early in the course of disease. After structural and neoplastic differentials are ruled out or considered, evaluation for differentials for which specific treatments (curative or palliative) exist should occur. These include parasitic causes (mites, nematodes, Cuterebra), infectious causes (viral rhinitis, fungal rhinitis), and allergic rhinitis. The goal of this approach is to arrive at a diagnosis of idiopathic chronic rhinitis with the knowledge that non-respiratory, anatomic, neoplastic, and potentially curable causes have been ruled out as much as possible, in order to maximize the likelihood of treatment success for a condition that is difficult and frustrating to manage. These tests are highly sensitive, particularly during active outbreaks, but may not detect latent viral infection during quiescent periods. Knowledge of this diagnosis early in cats can offer important prognostic information to clients. In many cases, however, useful, and even diagnostic information can be obtained from a single, straight, intra-oral, dorso-ventral or ventro-dorsal radiograph. This view allows for the assessment of symmetry or asymmetry between the left and right nasal cavities, turbinate loss, mass effect, and nasal foreign bodies, and can help to limit differential diagnoses. Rhinoscopy Nasal endoscopy provides a detailed visual assessment of the nasal airspace and mucosal surfaces. Because of the strong nasal irritant reflex, rhinoscopy should only be performed under general anesthesia. Retroflex nasopharyngoscopy is typically performed with a flexible endoscope placed in the oropharynx and flexed 180� over the soft palate, or using a rigid endoscope with a reverse offset. Endoscopic views of the nasopharynx and caudal nasal cavity can be enhanced by retracting the soft palate rostrally with a spay hook and directing the endoscope dorsally and rostrally into the nasopharynx. Anterior rhinoscopy is best performed with a rigid arthroscope or cystoscope directed through the nares into the left and right nasal cavities. In addition to providing a direct visual assessment of the nasal cavity, rhinoscopy can also be used to guide diagnostic sampling of the nasal cavity (samples for cytology, histopathology), and can also be used for therapeutic intervention. Diagnostic Nasal Sampling Because of the risk of potential complications, a lack of specialized equipment, and uncertainty about indications and interpretation of results, many practitioners consider diagnostic sampling of the respiratory system to be a daunting task. However, for many causes of nasal disease, there exist no pathognomonic hematologic or radiographic findings, making cytologic or histopathologic evidence of the condition the gold standard for diagnosis. With potential risks (chronic antibiotic therapy, steroidal or non-steroidal anti-inflammatory, immunosuppressives) and potential costs (inhalational therapy) associated with empirical and symptomatic therapy, a specific diagnosis should be sought whenever possible. There are several techniques available that will allow the safe and successful collection of samples for cytologic, histopathologic, and microbiological analysis in a general practice setting. Diagnostic samples from the nasal cavity and nasopharyngeal meatus should always be collected from anesthetized patients.
Endocranial complications drainage acne wiki order tretinoin cream from india, craniotomy or image guided aspiration as needed acne x ray discount 0.05% tretinoin cream with visa, are usually required for successful treatment (451 skin care 45 years old buy discount tretinoin cream 0.05% online, 452). Combined Intracranial complications may present with drainage of the paranasal sinuses (often the frontal sinus) can be performed endoscopically (448), albeit is in no way as a substitute non-specifc symptoms and signs (high fever, for the drainage of the intracranial abscess (447). Pathogens headache, lethargy, reduced consciousness) or with focal neurologic or increased intracranial most commonly involved in the pathogenesis of endocranial complications are Streptococcus and Staphylococcus species pressure signs and anaerobes (404, 451). Cavernous sinus thrombosis meningitis, cerebritis, and superior sagittal and cavernous sinus When the veins surrounding the paranasal sinuses are afected, thrombosis (231, 404, 412, 417, 435, 444). The clinical presentation of these complications can be non Such a complication has been estimated at 9% of intracranial specifc, being characterized simply by high fever with severe, complications (444, 445) and is a fortunately rare and dramatic intractable headache, or even be silent (411, 442). Intracranial abscesses are often heralded by signs of pain behind the orbit, complete ophthalmoplegia, papilloedema increased intracranial pressure, meningeal irritation, and focal and signs of meningeal irritation associated with spiking fevers neurologic defcits, including third, sixth or seventh cranial and prostration (425). Although an intracranial abscess can blood cell count with neutrophilia and polymorphotcytosis, while be relatively asymptomatic, subtle afective and behavioural lumbar puncture may show non specifc meningeal infammation changes often occur showing altered neurologic function, and blood cultures will help to culture the ofending organism altered consciousness, gait instability, and severe, progressive (445). N Complications Mortality / further defects Hansen 2011 (232) 16 9 subdural empyema Mortality 19% 3 meningitis Morbidity 19% 2 epidural abscess 2 intracerebral abscess 1 encephalitis 1 superior sagittal sinus thrombosis DelGaudio 2010 (447) 23 8 epidural Mortality 4% 10 subdural Morbidity 12% 2 intracerebral abscesses 3 meningitis Bayonne 2009 (412) 25 Epidural abscesses Sequelae 16% Subdural abscesses Mortality 0% Meningitis Germiller 2006 (448) 25 13 epidural abscesses Morbidity 8% (mean age 13 y) 9 subdural abscesses Mortality 4% 6 meningitis 2 encephalitis 2 intracerebral abscess 2 cavernous sinus thrombophlebitis Quraishi 2006 (449) 12 2 frontal lobe abscess Mortality 8% (mean age 14 y) 8 subdural abscess Morbidity 16 % 1 subdural abscess 1 2 cavernous sinus thrombophlebitis 2 Oxford 2005 (407) 18 7 epidural abscess No mortality (mean age 12 y) 6 subdural abscess Morbidity 11% 2 intracerebral abscess 2 meningitis 1 cavernous sinus thrombosis Younis 2002 (408) 39 7 epidural abscess Sequelae 10% 4 subdural abscess No mortality 21 meningitis 4 intracerebral abscess 1 superior sagittal sinus thrombosis Jones 2002 (440) 47 Subdural abscess 38% Mortality 2% Meningitis 2% Morbidity 19% Epidural abscess 23% Intracranial abscess 30% Albu 2001 (444) 16 6 meningitis Mortality 6% 6 frontal lobe abscess Morbidity 25% 5 epidural abscess 4 subdural abscess 2 cavernous sinus thrombosis Gallagher 1998 (445) 15 Meningitis 18% Mortality 7% Cerebral abscess 14% Morbidity 13% Epidural abscess 23% Clayman 1991 (413) 24 Meningitis 29% Mortality 4% Cerebral abscess 46% Morbidity 33% Epidural abscess Subdural abscess 8% Cavernous sinus thrombosis 8% Sagittal vein thrombosis 4% absence of venous fow in the afected cavernous sinus. No data are available for the infammation and are likely to be helpful, administered with paediatric population in which the mortality rate for intracranial concomitant antibiotics. Bone complications antibiotics administration and surgical debridement of Sinus infection can also extend to the bone producing sequestered bone and drainage (425). The most common osseous complications are ophthalmologist in cases of orbital involvement osteomyelitis of the maxillary (typically in infancy) or frontal and of neurologist/neurosurgeon in intracranial bones (398). On the anterior wall it presents clinically with �doughy� oedema of the skin over the frontal bone producing 3. Follow-up of complications a mass (Pott�s pufy tumour) whereas from the posterior wall It is important to note that some complications may spread occurs directly or via thrombophlebitis of the valveless occasionally appear simultaneously (for example Potts Pufy diploic veins leading to meningitis, peridural abscess or brain tumour and intracranial extension, orbital and intracranial abscess (425). A follow up of such patients for a minimum of 6 months is advised, in order to monitor for complete resolution In this context, Gallagher (445) reviewed the fles of 125 patients of disease as well as exclude disease recurrence or any with complicated rhinosinusitis and found that osteomyelitis complication of treatment. In the children Signs and symptoms of intracranial involvement are soft tissue where this illness is not self-limited and extends beyond oedema (especially of the superior lid), high fever, severe 7-10 days, many agree that a bacterial infection is likely. The headache, meningeal irritation, nausea and vomiting, diplopia, diagnosis is mostly based on history of symptoms and their photophobia, papillary oedema, coma and focal neurological duration as well as physical fndings. Whether this beneft outweighs the risks though contraindicated if intracranial pressure is elevated, can associated with frequent antibiotic prescriptions remains to also be useful. Ancillary therapy in the form of nasal Study Complication irrigations, antihistamines, decongestants, or mucolytics have Author, Year not been shown to be helpful. Because some younger children might not an initial milder phase of illness) (see also chapter 2). Their size than 7 days and abnormal fndings in the maxillary sinuses on continues to increase into the late teens and more than 85% of Water�s projection. The maxillary sinuses are who had symptoms for an average of 6 days before scanning usually pneumatized at birth and the volume in patients at 2 (467). Approximately 60% of the children had abnormalities years of age is around 2 ml (466). The sinus grows rapidly reaching in their maxillary and ethmoid sinuses, 35% in the sphenoid around 10 ml in volume around age 9 years and full growth sinuses, and 18% in the frontal sinuses. By adulthood, the foor of the maxillary reinforces the notion that, like in adults, every upper respiratory sinus is usually 4-5 mm inferior to the foor of the nasal cavity. By symptoms for >10 days without improvement (nasal discharge, the late teens, most of the sphenoid sinuses have aerated to the daytime cough worsening at night) or an abrupt increase in dorsum sellae and some further enlargement may occur in adults. Peak size was between 7 and 10 years of age and largest dimensions were In a longitudinal study of 112 children aged 6-35 months, in the 4-15 years age group. Based on those criteria, in children over 24 months, and 10% in children who were rhinosinusitis was confrmed in 89. The authors calculated the percentage of children in younger patients (2-5 years age group) whereas isolated experiencing symptoms beyond 2 standard deviations from rhinosinusitis was more frequent in older children. This value varied with age and was made as one would expect drainage from the sinuses to ranged between 16 and 22 days. The incidence based on these involve the adenoids as it moves posteriorly in the nose, and the assumptions ranged between 4 and 7. They reported that instead of the common bacteria noted Adenoiditis can have a very similar clinical presentation above, S. The predominant anaerobic 50 Supplement 23 bacteria were gram-negative bacilli such as Peptostreptococcus the recommendations of the American Academy of Paediatrics, and Fusobacterium (477, 478).
Allergen immunotherapy is effective for the treatment of overall clinical response does not appear to acne free reviews buy tretinoin cream cheap online vary signifi allergic rhinitis acne attack cheap tretinoin cream 0.025% on line. Allergen immunotherapy should be considered for patients topical potency skin care kit buy tretinoin cream discount, lipid solubility, and binding affinity. Intranasal corticosteroids may be useful in the treatment of specific IgE antibodies to clinically relevant allergens, and some forms of nonallergic rhinitis. Intranasal corticosteroids when given in recommended duced by avoidance and medication, the amount and type of doses are not generally associated with clinically significant medication required to control symptoms, and the adverse systemic side effects. Allergen immunotherapy may prevent the development of use of intranasal corticosteroids, nasal irritation and bleeding new allergen sensitizations and reduce the risk for the future may occur. Although there is no surgical treatment for allergic rhinitis, propriate for the treatment of very severe or intractable nasal surgery may be indicated in the management of comorbid symptoms or to treat significant nasal polyposis. However, conditions, such as nasal obstruction from severe nasal single administration of parenteral corticosteroids is discour septal deviation or inferior turbinate hypertrophy, adenoidal aged and recurrent administration of parenteral corticoste hypertrophy, or refractory sinusitis and complications roids is contraindicated because of greater potential for thereof. Management and monitoring of rhinitis should be individu prevention and treatment of allergic rhinitis and is associated alized and based on the spectrum, duration, and severity of with minimal side effects. C Consultation with an allergist/immunologist Education of patient and caretakers 108. Education is a key element in promoting adherence and op however, consultation/referral services are often under timizing treatment outcomes in allergic rhinitis. Consultation with an allergist/immunologist should be con Major comorbid conditions sidered for patients with rhinitis who have inadequately 95. Treatment of allergic rhinitis may improve asthma control in tify the allergens to which they are sensitized and to receive patients with coexisting allergic rhinitis and asthma. There is no established cause-and-effect relationship of rhi such as asthma and recurrent sinusitis, or when allergen nitis with recurrent otitis media and otitis media with effu immunotherapy is a consideration. Rhinitis is usually associated with infiam hort and case-control studies as well as birth registry data mation, but some forms of rhinitis such as vasomotor rhinitis or before reaching a decision. The most critical time for concern about potential congenital frequently is accompanied by symptoms involving the eyes, ears, malformation because of medication use is the first trimes and throat. A sufficient amount of human observational data has now been accumulated to demonstrate safety for second-gener Classification and differential diagnosis of rhinitis ation as well as first-generation antihistamines. Topical decongestants when used on a short-term Rhinitis is classified as allergic or nonallergic, but not all types basis may have a better safety profile than oral agents for of rhinitis can be easily separated into one of these categories. Sodium cromolyn is a safe treatment for allergic rhinitis allergic and nonallergic because it may have components of both during pregnancy. Montelukast is a safe treatment for allergic rhinitis during of rhinitis include nasal polyps, cerebrospinal fiuid rhinorrhea, pregnancy. In an attempt to do this, an international working group 9 ing pregnancy but without dose escalation. This classification system discarded the terms seasonal and common in other age groups but may also be infiuenced perennial, emphasizing that an aeroallergen (eg, grass pollen) that by age-related physiologic changes such as cholinergic hy occurs seasonally in one region may be detected throughout the peractivity, anatomic changes, and medications taken for year in another geographical area. C rhinitis may be a useful comparative reference point for other se verity grading schemes; this states that none of the following items is present: sleep disturbance; impairment of daily activities, lei Athletes sure, and/or sport; impairment of school or work; and symptoms 107. Athletic performance can be affected by rhinorrhea and 11 present but not troublesome. In this document, the Joint Task Force retains and uses the terms seasonal and perennial in classifying patients with allergic rhinitis. Children with a bilateral family history of atopy may develop symptoms more frequently and 6,25 glucocorticoids effectively reduces eosinophils and the release at a younger age than those with a unilateral family history. Aeroallergen sensitization rarely begins before 6 months of age 27 When allergen challenges are given repeatedly, the amount but may start between 6 months and 2 years of life. Food ingestion rarely causes allergic rhinitis Consequently, at the end of a pollen season, symptoms may de in infants, children, or adults unless there are associated gastrointes cline at a slower rate than the pollen count. The prevalence of tant to know the full spectrum of aeroallergens to which the patient seasonal allergic rhinitis is higher in children and adolescents, 31 responds as well as seasonal variations in symptoms. As in patients with asthma, early-phase and late-phase re sponses may be seen in allergic rhinitis. Mediators released from eosinophils during the late associated ocular allergy symptoms in controlled trials.
For diagnostic reasons acne makeup discount tretinoin cream american express, testing is recommended to skin care 40s 0.05% tretinoin cream with amex be done above and below these frequencies to skin care blog purchase tretinoin cream 0.025% on-line more thoroughly map the ability of the ear to perceive sound and to indicate minimal losses of which the examinee is unaware but which may be early symptoms of inner ear disease. After finding the threshold for 1 000 Hz, the higher frequencies are tested in the same manner and in ascending order (2 000, 3 000, 4 000, 6 000 and 8 000 Hz). Then the ear selector switch is turned to the opposite ear and the sequence is repeated. Masking is especially important in taking bone conduction measurements, and it should be used with both tuning fork and audiometer examinations. The greater the discrepancy in hearing between the ears, the greater the need for masking the better ear. Audiometers are equipped with a masking sound (a mixture of frequencies, sometimes called "white" noise). The intensity generally ranges from -20 to +100 dB, and the frequency ranges from 125 to 8 000 Hz. Pure tone audiometry should be carried out in a quiet room in which the background noise intensity is less than 35 dB(A), i. It produces the spoken voice rather than pure tones at controlled intensity levels. The percentage of words correctly perceived, independently of the type of material used, gives the intelligibility rate (articulation score). Tests should aim at an assessment of strictly auditory functions and not depend on the ability to grasp the meaning of codes and sentences heard incompletely, as in unfamiliar situations dangerous misunderstandings from incorrect interpretation might occur. The following material is used in several States for testing speech intelligibility, listed in order of increasing difficulty: 12. No matter how loud P-B words are presented, the examinee with severe inner ear hearing loss fails to make an adequate score. Speech is essentially compressed into this range, which is sufficient for fairly complete understanding. This is the person who will often remark, �I can hear you, but I can�t understand you�. These individuals have difficulty in group conversation or when listening against a background of noise. Flight safety under these conditions is not impaired as long as it is made certain in each case that intelligibility of speech and perception of signals under background noise, as well as hearing on the ground for briefing and check-list procedures is satisfactory (Annex 1, 6. Voice communications between crew members in the cockpit including instructions and routine check-list operations must be clearly understood, also during approach, landing and emergency operations. The volume of the test material should be controllable by the applicant in a manner representative of the aircraft communication equipment. Head-shadow effects, brought about by the head in certain positions, cause poorer discrimination during monaural reception and might affect efficient communication between crew members and should be taken into account. The differences in signal-to-noise ratio necessary for equivalent monaural and binaural perception are usually 3�4 dB. Monaural hearing in both private pilots and professional flight crews should therefore always be investigated and evaluated in accordance with best medical practice as well as assessed under 6. Here the auditory signals are picked up by a microphone placed beside the poor ear and shunted across, either electrically or acoustically, to the good ear. A non-occluding-type ear mould is used in the good ear which permits the direct reception of auditory stimuli in that ear. There are, however, quite a number of flight crew who can benefit, particularly socially, by an aid. These carbon-type aids were responsible for the prevalent notion that only persons with conductive hearing loss could benefit from hearing aids. The development of the transistor and the transistor hearing aids opened up a new era in design and fitting. By testing appropriately powered aids with frequency response characteristics deemed suitable for the particular hearing loss involved, it is often possible to demonstrate clear-cut and significant improvements in performance. Arguments against the use of hearing aids for licensing purposes centre around their delicate nature, their relatively low reliability, and their suboptimal acoustic performance. However, personal hearing aids are not normally required in flight because of the mandatory aircraft intercom and radio equipment. The best aids presently available provide a maximum of approximately 70 per cent of normal speech perception in environments of even relatively low ambient noise. This results from the frequency-response characteristic of aids, which is not �flat� in the 500 to 3 000 Hz range (as in the normal ear�s response) and which above 3 000 Hz shows deep �valleys� in which ambient noise intrudes, masking adjoining frequencies.
Order discount tretinoin cream on line. How To Take Care Of Your Skin Before Wedding | Skin Care Tips Before Wedding | Foxy Makeup.