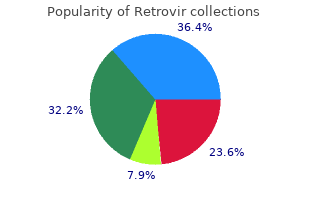
Retrovir
"Discount 300mg retrovir with visa, medicine keri hilson lyrics".
By: A. Dargoth, M.B. B.CH. B.A.O., M.B.B.Ch., Ph.D.
Clinical Director, Mayo Clinic College of Medicine
The endovascular approach has been shown to have a lower short-term mortality medicine while breastfeeding buy generic retrovir 300 mg on line, but this advantage is lost over time because of the incidence of graft failure symptoms 10dpo effective 300mg retrovir. They are described based on their location within the thoracic aorta: the aortic root chapter 7 medications and older adults retrovir 100 mg otc, the ascending thoracic aorta, the aortic arch, or the descending thoracic aorta. They can also obstruct the superior vena cava if they are large, resulting in distended neck veins on examina- tion. Findings include a widened mediastinum, tracheal deviation, and enlargement of the aortic knob. D-Dimer in ruling out acute aortic dissection: a systematic review and prospective cohort study. Serum D-dimer is a sensitive test for the detection of acute aortic dissection: a pooled meta-analysis. Young adult patients with short dissec- tion length and thrombosed false lumen without ulcer-like projections are liable to have false-negative results of D-dimer testing for acute aortic dissection based on a study of 113 cases. Sensitivity of the aortic dissection detection risk score, a novel guideline-based tool for identification of acute aortic dissection at initial presentation: results from the International Registry of Acute Aortic Dissection. Nonsurgical reconstruction of thoracic aortic dissection by stent-graft placement. Meta-analysis of open versus endo- vascular repair for ruptured descending thoracic aortic aneurysm. Utility of the aortic fenestration technique in the management of acute aortic dissections. Long-term outcomes of surgical aortic fenestration for complicated acute type B aortic dissections. Screening for abdominal aortic aneurysms: single centre randomised controlled trial. Analysis of cost effectiveness of screening Danish men aged 65 for abdominal aortic aneurysm. Screening men for abdominal aortic aneurysm: 10 year mortality and cost effectiveness results from the randomised Multicentre Aneurysm Screening Study. Screening for abdominal aortic aneurysm: a best-evidence systematic review for the U. Long-term benefit and cost- effectiveness analysis of screening for abdominal aortic aneurysms from a randomized controlled trial. Emergency department ultrasound scan- ning for abdominal aortic aneurysm: accessible, accurate, and advantageous. Prospective study of accuracy and outcome of emergency ultrasound for abdominal aortic aneurysm over two years. Outcomes following endovascular vs open repair of abdominal aortic aneurysm: a randomized trial. Yearly rupture or dissection rates for thoracic aortic aneurysms: simple prediction based on size. Surgical intervention criteria for thoracic aortic aneurysms: a study of growth rates and complications. Natural history of thoracic aortic aneurysms: indications for surgery, and surgical versus nonsurgical risks. Whittingham Department of Molecular Biology and Medicine, Monash University, Clayton 3168, Australia; E-Mail: senga. Although a pathogenic role has been demonstrated for various autoantibodies reactive with cell surface and extracellular autoantigens, studies using monoclonal antibodies (mAb) show not all antibodies in the polyclonal response are pathogenic. Differences depend on Fab-mediated diversity in epitope specificity, Fc-mediated effects based on immunoglobulin (Ig) class and subclass, activation of complement, and the milieu in which the reaction occurs. In vitro they may inhibit or adversely affect well-defined intracellular biochemical pathways, yet, in vivo they are separated from their autoantigens by multiple cellular barriers. Recent evidence that Ig can traverse cell membranes, interact with intracellular proteins, and induce apoptosis has provided new evidence for a pathogenic role for such autoantibodies. Keywords: autoimmune disease; monoclonal antibody; immunoglobulin; epitopes; Fc receptors; intracellular antigens; autoantibodies Antibodies 2015, 4 315 1. Introduction the first description of a pathogenic autoantibody by Donath and Landsteiner in 1904 [1] was a landmark discovery in the history of clinical medicine. For the second half of the 19th century clinicians had grappled with the definition of a condition that was characterized by “paroxysms” induced by cold and followed by hemoglobinuria. Typically, but not exclusively, these episodes occurred in subjects with syphilis.
Beforehand medications used for bipolar disorder order retrovir mastercard, explanations on the purpose and how the information will be used and the opportunity for questions and preferences needs to be provided medicine man buy genuine retrovir on-line, permission sought and scales and tape measures adequate treatment management company safe retrovir 300mg. Implications of results need to be explained and where this impacts on emotional wellbeing, support provided. However off label use is predominantly evidence-based and is allowed in many countries. Where it is allowed, health professionals need to inform women and discuss the evidence, possible concerns and side effects of treatment. Variable availability and regulatory status of these agents is notable and for some agents, potential liver toxicity requires caution. Where off label use of ovulation induction agents is allowed, health professionals need to inform women and discuss the evidence, possible concerns and side effects. If pregnancy occurs, the following need to be considered: Awareness and preventative management of pre-and post-operative nutritional deficiencies is important, ideally in a specialist interdisciplinary care setting Monitoring of fetal growth during pregnancy. Off-label pre- scribing occurs when a drug is prescribed for an indication, a route of administration, or a patient group that is not included in the approved product information document for that drug by the regulatory body. Prescribing off-label is often unavoidable and common and does not mean that the regulatory body has rejected the indication, but more commonly there has not been a submission to request evaluation of the indication or that patient group for any given drug. Our collaborating and engaged societies and consumer with international expert panels, and e-health information groups: resources available at . Costello has declared shares in Virtus Health and past spon- Italian Society of Gynaecology and Obstetrics sorship from Merck Serono for conference presentations. Marie Misso Melanie Gibson-Helm, Monash University, Australia led the guideline development and evidence synthesis pro- Cheryce Harrison, Monash Centre for Health Research cesses. Polycystic ovary syndrome: a complex condition Edgar Mocanu, Royal College of Surgeons, Rotunda Hos- with psychological, reproductive and metabolic manifestations that impacts on health across the lifespan. Delayed diagnosis University of Hong Kong, Hong Kong and a lack of information associated with dissatisfaction in women Sharon Oberfield, Columbia University Medical Center, with polycystic ovary syndrome. Fertil Steril 2017;107(6): Alexia Pena, the Robinson Research Institute at the Uni-~ 1380–6. Polycystic ovary syndrome: Jie Qiao, Peking University Third Hospital, China perceptions and attitudes of women and primary health care physicians on features of pcos and renaming the syndrome. J Clin Endocrinol Metab Leanne Redman, Pennington Biomedical Research 2014;99(1):E107–11. Diagnosis and treatment of polycystic ovary syndrome: an Endocrine Society clinical practice guideline. Tapanainen, University of Helsinki, Helsinki Uni- from the European Society of Endocrinology. Assessment and management of polycystic ovary syndrome: Summary of Implementation, Australia an evidence-based guideline. Department of Social Medicine, its associated complications in Iranian women using meta-analysis method. Data were analyzed using a random-effects model meta-analysis Medical Sciences, Ilam, Iran. Results: 30 studies conducted between the years 2006 to 2011 were entered into meta-analysis. Malihe Akbari, Department of Also, the prevalence of hirsutism was estimated to be 13%, acne 26%, androgenic Nursing and Midwifery, Ilam alopecia 9%, menstrual disorders 28%, overweight 21%, obesity 19%, and infertility University of Medical Sciences, 8%. Received: 5 July 2014 Revised: 22 November 2014 Accepted: 21 June 2015 Key words: Polycystic ovary syndrome, Prevalence, Hirsutism, Acne, Obesity. The main the most common endocrine complications of the disease in adolescence Pdisorder in women of reproductive are the incidence of amenorrhea, oligo age and is the most common cause of menorrhea, hirsutism, obesity, and acne. Various studies fertility ages, the patient’s chief complaint is have reported a prevalence of 5-10% for infertility and irregular ovulation. It appears that several factors menopausal ages, this syndrome can may be involved in its development. Perhaps increase the risk of type 2 diabetes, the disease exists as a genetic predisposition hypertension, dyslipidemia, cardiovascular in the person and its symptoms are diseases and even endometrial cancer and exacerbated by environmental factors and possibly breast cancer (4). The first disease, and increased risk of endometrial, definition was proposed by the National uterine, and breast cancers. The second definition clinical or laboratory hyperandrogenism in (Rotterdam) was presented by Fertility and which these items are used in clinical Embryology Association of Europe and diagnosis (5). Clinical hyperandrogenism: (acne, Clinical hyperandrogenism symptoms include hirsutism, and androgenic alopecia) or symptoms such as hirsutism, acne, biochemical hyperandrogenism (elevated androgenic alopecia, and incidence of male serum androgen levels).
Though significant progress has been made over the past decade in uncovering unique valve cell biology and pathogenic mechanisms medicine to stop vomiting order discount retrovir, what we have learned is very much a beginning section 8 medications discount retrovir 300mg otc. This knowledge gap is a principal impediment to creating new therapies for valve disease symptoms quad strain discount 300mg retrovir amex. In this review, we summarize what is known about aortic valve biology, pathogenesis, clinical management, and regeneration and propose future research directions. Aortic valve structure and physiology the aortic valve is composed of three semilunar cusps (also called “leaflets”) attached to a fibrous annulus connected to the distal end of the left ventricular outflow tract. A portion of the annulus is attached to cardiac muscle, while the other half is continuous with the fibrous leaflet of the mitral valve. The functional unit of the valve, however, includes the cusps and their respective aortic sinus complexes, the latter collectively called the aortic root. Root structure the aortic root is a bulb-shaped fibrous structure to which the aortic cusps, or leaflets, are attached. The sinuses of Valsalva are three elliptical depressions in the aortic wall opposite each leaflet, with. The cusps attach valve consists of a rigid root (R) with three compliant cusps (C). B) the root wall to the annulus with a parabolic profile, meeting at commissure points. Modified from C) the coronary artery ostia (O) originate within the aortic root sinus (S). The root is populated with blood-vessel like endothelial, medial smooth muscle, and adventitial fibroblasts. These layers appear to vary in relative thickness, which suggests regional dif- cusps are virtually avascular, being thin enough (b1 mm) to receive ference in tissue biomechanics, but to date these have not been nourishment through hemodynamic convection and diffusion [7–9]. Coordinated function aortic root wall cells are partly derived from neural crest and anterior heart field sources (reviewed in [1,2]). Genetic or surgical deletion of the aortic valve leaflets function in concert with the aortic root to these progenitor cell fields results in outflow tract malformations, maintain efficient cyclic opening and closing. The leaflets are including truncus arteriosus and transposition of the great arteries mutually apposed during diastole, and a small overlap of leaflet tissue, (reviewed in [3]). Understanding the physiological and pathological called the lunula, ensures a closed volume for efficient filling of the left mechanisms of this heterogeneous and transient cellular composition ventricle. The valve annulus expands during this time, pulling the in developing aortic valves is a major focus of developmental biology leaflets taught to prevent prolapse [10]. Valve cusp structure stellate orifice results, even without the presence of transvalvular flow [11]. Thevalveorifice changes quickly from stellate, to triangular, to the valve cusps are very thin, flexible structures, which come to- finally a circular pattern as blood is ejected from the ventricle, opening gether to seal the valve orifice during diastole. Theaorticrootadjustsfrom subdivided into three distinct layers: the fibrosa, ventricularis, and a conical to a cylindrical shape during ejection, providing optimal spongiosa[5]. Thefibrosaislocatedontheaorticsideoftheleaflet,andis hemodynamics at the larger flow volume [12]. The aortic valve closes composed of collagen sheets and large bundles arranged in the much more gradually relative to opening, the dynamics depending on circumferential direction with very little elastin [6]. The thinner the transvalvular pressure and the parameters of the vortexes that ventricularis covers the ventricular surface of the leaflet, and has develop within the sinuses of Valsalva. The reduction of forward blood considerably more elastin than the fibrosa, but both components are velocity causes a bifurcation of the flow field to develop, and part of the organized with somewhat less directionality than in the fibrosa when flowcirculates behindtheleaflets,creatinga vortex [13]. A) the root and cusps undergo dynamic anisotropic deformation with each heartbeat. B) Biaxial mechanical testing of fresh and gludaraldehyde treated aortic valve leaflets. C) Role of elastin and collagen microstructure in mediating valve cusp deformation. In vivo kinematics because the effects of multiaxial collagen fiber distributions in the cusp will remain intact and therefore testable [27,28]. Generally, the majority of the stresses and strains experienced by the leaflets cusps extend very compliantly until reaching a critical strain occur during diastole and early opening of the valve. Uniaxial test results suggest the elastic mation based on elementary beam mechanics [14]. This increased More careful considerations of the geometry of the load bearing compliance is likely due to changing cross-fiber recruitment and surfaces during systole and diastole have generated estimates of splay [27].
Syndromes
- Immunoglobulin testing
- Check your blood pressure
- Restlessness when awake
- Dementia that rapidly worsens over a few weeks or months
- Fainting or feeling light-headed
- Meat, poultry, eggs,milk and other dairy foods
- Eat more slowly
- Achondroplasia
Such programs are appropriate for prevention nioxin scalp treatment buy cheap retrovir 300mg online, before the patient is entrenched in a chronic pain syndrome or before severe pain and illness behavior evolves medicine allergy best buy for retrovir. Recommendation: Work Conditioning medications used to treat depression buy retrovir mastercard, Work Hardening, or Early Intervention Programs for Chronic Knee Pain Syndromes Work conditioning, work hardening, and early intervention programs are recommended for treatment of chronic knee pain syndromes. Frequency/Duration – Three (3) to 5 times a week for work conditioning and early intervention programs; daily for work hardening. Weekly evaluations demonstrating sufficient levels of physical effort and consistency, compliance with the plan of care, and functionally significant progress toward the return-to-work goal must be documented to justify continuation. Program length and intensity is dictated by each patient’s unique rehabilitation needs. Strength of Evidence Recommended, Insufficient Evidence (I) Rationale for Recommendation There are no quality studies of knee pain patients and limited evidence that work conditioning, work hardening, or early intervention programs are effective for chronic spinal pain, nevertheless there is a longstanding belief and experience that they are highly effective. While there is potential for overlap, work conditioning, work hardening, and early intervention are distinct programs and are not intended for sequential use, although this might be appropriate in certain situations depending on program components. In acute cases, where delayed recovery is not an issue, these programs are inappropriate. Program choice depends on availability and matching patient needs to the services offered to provide the most cost-effective and beneficial outcome. Hence, these programs might provide the greatest potential impact when used to manage patients during the subacute phases of injury, although they might also be appropriate for use in those with chronic pain who do not, after evaluation, have significant psychosocial factors contributing to their clinical presentation. Evidence for the Use of Work Conditioning, Work Hardening, and Early Intervention Programs There are no quality studies evaluating the use of work conditioning, work hardening, and early intervention programs for chronic knee pain. These programs are intended to manage psychological, social, physical and occupational factors and are discussed in detail in the Chronic Pain guideline. This team may include physical and occupational therapists, psychologists, vocational counselors, nurses, and case managers. Quality programs emphasize functional recovery and active, progressive physical activity and generally involve intensive 5-days-a-week treatment regimens that should be individualized. All medical and therapy services must be supervised by a physician who is directly involved with the program and regularly interviews and Copyright 2016 Reed Group, Ltd. For reasons that are unclear, there appear to be few lower extremity pain patients, including knee pain patients who require these programs. Nevertheless, a minority of patients may derive benefits (see Chronic Pain guideline). Indications – Chronic knee pain in patients who are not working, or unable to return to full duty, and have significant, pain-related limitations in activities of daily living. Frequency/Duration – Median 20 days, with trial of the first 10 days to assess patient compliance, attendance, and progress. Complicating problems involving activities of daily living (such as coordinating part-time employment, transportation, or child care needs) or limitations imposed by co-morbid medical conditions which preclude the patient from participating in the program full-time (thus preventing them an assessment at 10 days) are considerations that might necessitate program modification. Indications for Discontinuation – Failure to improve, noncompliance, resolution of symptoms and disability, exhaustion of reasonable program duration for a specific condition. These programs may be helpful if there is medical need to wean the patient from opioids or other medications and/or if the patient has shown demonstrable clinical progress with less intense rehabilitation but “pain limitation” has impeded adequate recovery. Development of entrenched psychosocial barriers to recovery and a chronic pain syndrome as sequelae of the original physical components of the injury may be associated with this group of patients. Functional restoration might be appropriate, as well as vocational re-entry in positions not requiring the same job physical characteristics when all previous treatments have failed. With the possible exception of workplace-based interventions, most successful multidisciplinary programs appear to utilize either a cognitive-behavioral approach or involve psychologists. However, there are times when earlier referral in the mid- to late-subacute interval is indicated. Referrals during the subacute phase best occur when there is a quality program with proven outcome efficacy is available, the patient has documented delayed recovery, yet there is interdisciplinary assessment that the patient is likely to benefit from the program. Only the recommendations are reviewed here, and the reader is referred to the Hip and Groin Disorders guideline for further details. Reported risk factors in these post-operative patients include age, general anesthesia, and obesity. While initially believed to be a complication of hospitalization, post-hospital discharge surveillance data suggest high risks of thromboembolism continue well after discharge,(1944) with many studies treating patients for 30 days for longer. Recommendation: Prevention of Venous Thromboembolic Disease Prevention of venous thromboembolic disease is strongly recommended for post- operative knee patients, particularly arthroplasty patients or other post-operative patients with prolonged reductions in activity. Recommendation: Compressions Stockings for Prevention of Venous Thromboembolic Disease the use of post-operative graded compression stockings is moderately recommended for the prevention of venous thromboembolic disease.
Cheap generic retrovir uk. Pet Care - Dehydration for Dog/Cats - Bhola Shola.