Zebeta
"Purchase cheapest zebeta and zebeta, blood pressure quiz pdf".
By: X. Deckard, M.B.A., M.B.B.S., M.H.S.
Associate Professor, University of South Carolina School of Medicine
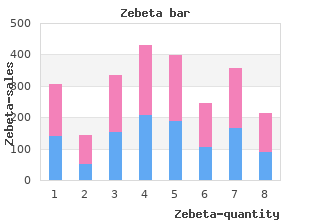
Given the renewed attention and likely heated debate that will follow this recent ruling arrhythmia vs fibrillation discount zebeta 10 mg overnight delivery, study the Massachusetts experience with mandated coverage is important hypertension yoga exercises cheap zebeta 10 mg visa. A retrospective review was performed within the department of orthopedics at a tertiary-care arteriovenous oxygen difference purchase zebeta without prescription, academic medical center in Massachusetts. The departmental billing database was queried to identify all International Classification of Diseases, Ninth Revision, Clinical Modification codes related to the knee. In an effort to validate the cohort, the ten most common diagnosis codes were identified for two periods in time: Pre-reform (calendar years 2005-2006) and post-reform (calendar years 2007-2010) periods for three orthopaedic surgeons. These ten diagnosis codes were then used to identify all new patients seen by three surgeons in pre-reform (2005-2006) and post reform (2007-2010) periods (n = 10420. Although the healthcare reform was passed on April 12, 2006, the law did not take effect until the beginning of 2007. In keeping with prior investigations, the calendar year 2006 was considered pre-reform[5,6]. To control for confounders, eligible patients were limited to those seeking care from three orthopaedic surgeons with established practices at one academic institution throughout both study periods. These different payers were grouped into four insurance groups (uninsured, government, private, Workers� Compensation) and seven insurance types (Medicaid, Medicare, Worker�s Compensation, private insurance, uninsured, Commonwealth Care, and TriCare) allowed for continuity with previous investigations[5,6]. In keeping with the method described by McGlaston et al[6], an effect size of greater than or equal to 10% in the rate of surgery was considered clinically significant. An a priori sample size analysis indicated that a 10% difference in the rate of surgery between insurance categories with an of 0. While gender did not significantly differ between the two study periods, comparison of the cohort�s demographics reveals several disparities (Table 1. Self-reported racial groups demonstrated a significant increase in �White� patients and significant decreases in �Other� and �Unknown/Unreported�. The highest level of education showed a significant increase in all groups except �I did not attend school� and �8th grade or less�. When divided into insurance subgroups, TriCare subgroup�s increase was statistically significant from 1% to 2% as was Medicaid�s statistically significant decrease post-reform from 10% to 9%. Mandated insurance increases knee surgery rates Table 1 Demographic characteristics of the pre and post-reform cohorts Pre-reform (n) (%) Post-reform (n) (%) P-value Total 2640 7780 Gender Female 1551 59% 4419 57% 0. Mandated insurance increases knee surgery rates Figure 1 Figure 1 Cohort distribution by payer group. Four insurance group rates of surgery: Pre-reform vs post-reform When the groups were compared by their type of insurance (uninsured, private, government-sponsored, and Workers� Compensation, no significant differences were found before and after healthcare reform (Figure 3. Seven insurance group rates of surgery: Pre-reform vs post-reform Insurance subgroup analysis further subdivided the patients within the government group into Medicare, Medicaid, TriCare, and Commonwealth Care. Each group�s rate of surgery pre-reform and post-reform was computed and compared using chi-square analysis. Rates of surgery across these six groups were not significantly different when compared between the two periods (Figure 4. It is hypothesis generating and suggests avenues for further research into mandated coverage within Massachusetts and nationally. This explanation assumes that there are patients without insurance with operative diagnoses that are now becoming surgical candidates because they are insured. This idea is supported by a significant decrease in the number of uninsured patients. It is possible that a musculoskeletal problem, which was neglected while a patient was uninsured, might require a surgery once they have coverage. Mandated insurance increases knee surgery rates Figure 2 Figure 2 Rates of Surgery Increased from 8. Despite starting with more than 10000 eligible patients, many of the subgroups (both insurance groups and type) had less than the recommended 300 individuals participating. Specifically, in the four sub-group analysis, the Workers� Compensation and uninsured categories were underpowered. In the seven sub-group analysis, all groups were underpowered, except the Medicare insurance group.
This training includes both didactic and clinical education and includes a demonstrated competency in pharmacology blood pressure medication extreme tiredness order 5mg zebeta free shipping. The spectrum of duties performed by an advanced practice registered nurse will vary according to the institution and may be determined by state regulations fetal arrhythmia 38 weeks 10mg zebeta for sale. Each institution should develop a procedure for the initial granting and subsequent maintenance of privileges arrhythmia breathing purchase zebeta 10mg otc, ensuring that the proper professional credentials are in place. Each institution must ensure that the advanced prac tice registered nurse has the formal education to function within the neonatal scope of practice. That procedure is best developed by the collaborative efforts of the nursing administration and the medical staff governing body. Clinical care by the advanced practice registered nurse for neonates receiving level I neonatal care is provided in collaboration with, or under the supervision of a physician with special interest and experience in neonatal medicine, usually this is a pediatrician or neonatologist. The number of staff and level of skill required are influenced by the scope of nursing practice and the degree of nursing responsibilities within an institu tion. Close evaluation of all factors involved in a specific case is essential for establishing an acceptable nurse�patient ratio. Variables, such as birth weight, gestational age, and diagnoses of patients; patient turnover; acuity of patients� conditions; patient or family education needs; bereavement care; mixture of skills of the staff; environment; types of delivery; and use of anesthesia must be taken into account in determining appropriate nurse�patient ratios. Perinatal nursing care in a facility at this level of care should be under the direction of a registered nurse. The registered nurse�s responsibilities include directing perinatal nursing ser vices, guiding the development and implementation of perinatal policies and procedures, collaborating with medical staff, and consulting with hospitals that provide higher levels of care in the region or system. For perinatal care, it is recommended that there be an on-duty regis tered nurse whose responsibilities include the organization and supervision of antepartum, intrapartum, and neonatal nursing services. The presence of one or more registered nurses or licensed practical nurses with demonstrated knowledge and clinical competence in the nursing care of women, fetuses, and newborns during labor, delivery, and the postpartum and neonatal periods is suggested. Ancillary personnel, supervised by a registered nurse, may provide support to the patient and attend to her personal comfort. Intrapartum care should take place under the direct supervision of a reg istered nurse. Responsibilities of the registered nurse include initial evaluation and admission of patients in labor; continuing assessment and evaluation of patients in labor, including checking the status of the fetus, recording vital signs, monitoring the fetal heart rate, performing obstetric examinations, observing uterine contractions, and supporting the patient; determining the presence or absence of complications; supervising the performance of nurses with less training and experience and of ancillary personnel; and staffing of the delivery room at the time of delivery. A licensed practical nurse or nurse assis tant, supervised by a registered nurse, may provide support to the patient and attend to her personal comfort. Inpatient Perinatal Care ServicesCare of the Newborn 3131 Postpartum care of the woman and her newborn should be supervised by a registered nurse whose responsibilities include initial and ongoing assessment, newborn care education, support for the attachment process and breastfeeding, preparation for healthy parenting, preparation for discharge, and follow-up of the woman and her newborn within the context of the family. This regis tered nurse should have training and experience in the recognition of normal and abnormal physical and emotional characteristics of the mother and her newborn. Again, a licensed practical nurse or nurse assistant, supervised by a registered nurse, may provide support to the mother and attend to her personal comfort in the postpartum period. Routine newborn care delivered by the registered nurse is provided in col laboration with a pediatrician. The nurse monitors the infant�s adaptation to extrauterine life and then, ideally, assists in the transition of the healthy new born to the mother�s room. Hospitals at this level of care should have a director of perinatal and neonatal nursing services who has overall responsibility for inpatient activities in the respective obstetric and neonatal areas. This registered nurse should have demonstrated expertise in obstetric care, neonatal care, or both. In addition to fulfilling basic perinatal care nursing responsibilities, nurs ing staff in the labor, delivery, and recovery unit should be able to identify and respond to the obstetric and medical complications of pregnancy, labor, and delivery. A registered nurse with advanced training and experience in routine obstetric care and high-risk obstetric care should be assigned to the labor, deliv ery, and recovery unit at all times. Licensed practical nurses and unlicensed personnel who have appropriate training in perinatal care and are supervised by a registered nurse may provide assistance with the delivery of care, provide support to the patient, assist with lactation support, and attend to the woman�s personal comfort. All nurses caring for ill newborns must possess demonstrated knowledge in the observation and treatment of newborns, including cardiorespiratory monitoring. The neonatal nurse at this level cares for premature or term newborns who are ill or injured from complications at birth. The neonatal nurse provides the newborn with frequent observation and monitoring and should be able to monitor and maintain the stability of cardio pulmonary, neurologic, metabolic, and thermal functions, either independently or in conjunction with the physician; assist with special procedures, such as lumbar puncture, endotracheal intubation, and umbilical vessel catheterization; and perform emergency resuscitation.
Cheapest generic zebeta uk. Calibrate your blood pressure monitor with phone.
Ligamentum Capitis Femoris � the capitis femoris ligament extends from the acetabular notch to the femur heart attack demi lovato order zebeta now. Normal Range of Hip Motion in the Adult � Hip flexion: 120� � Hip extension: 30� � Hip abduction: 45�50� � Hip adduction: 0�30� � External rotation of the hip: 35� � Internal rotation of the hip: 45� � Osteoarthritis will limit internal rotation of the hip first blood pressure chart meaning zebeta 10 mg visa. Thomas� Test (Figure 4�78) � this test is used to assess hip flexion contractures arrhythmia yahoo answers buy 5 mg zebeta amex. Apparent Leg Length Discrepancy (Figure 4�82) � First determine that no true leg length discrepancy exists. Clinical Features � Pain associated with piriformis injury may present in the lateral buttock, posterior hip, and proximal posterior thigh, as well as the sacroiliac region. Imaging � Radiographs of the low spine and hip may be necessary to rule out other pathologic causes of pain. Patient may also have tenderness over ante rior groin/inferior abdomen with ilipsoas tendonitis. Provocative Tests � External snapping hip syndrome: internally and externally rotate the hip passively while the patient is in the lateral decubitus position. Clinical Features � Presents as pain in the adductors distal to their origin at the ramus or adductor tubercle. Imaging � Radiographs of the hip including the adductor tubercle to rule out avulsion. Note relationship of the trochanteric bursa between Clinical Features the iliotibial band and the greater trochanter (anterior view. Essentials � Patients report night pain and are unable to of Musculoskeletal Medicine. The knee strikes the dashboard with the femur in this position, driving it posteriorly. In this position, the head of the femur is covered posteriorly by the capsule and not by bone. Imaging � Hip radiographs Treatment � this is an orthopedic emergency due to potential vascular compromise and sciatic nerve injury. Treatment � the main objective is to maintain the femoral head within the acetabulum while healing and remodeling occurs. Note: the risk for pulmonary embolism is highest during the second and third week. Imaging � Radiographs of the hip � Bone scan may be necessary for occult fractures. Prompt reduction under general anesthesia will most likely preserve the replacement. Clinical Features � the typical signs and symptoms of hip fracture are present: hip pain with an external rotated limb with possible shortening and malalignment. Clinical Features � Femoral-neck stress fractures present as groin pain made worse with activities of daily living. Imaging � Radiographs may be negative at first and in time may show periosteal thickening or a radiolucent line. Treatment � Compression type � Because they are more stable, they may be treated with bedrest. Treatment � Generally, this avulsion is treated with rest, ice, and weight bearing as tolerated. Clinical Features � Osteitis pubis presents as pubic symphysis or groin pain and may radiate into the thigh. Clinical Features � There will be pain and a palpable mass at the site of the lesion. Treatment � Gentle range of motion � Prevention of contractures is of prime importance. It is susceptible to injury because it is at the end of the tibia and femur, 2 long lever arms. Bony Anatomy (Figure 4�93) � the knee can be divided into the medial femoral tibial, lateral femoral tibial, and patellofemoral regions. Tibial Plateau � Characterized by curved surfaces cor responding to the medial and lateral femoral condyles.
Pregnancy in women with b-thalassemia major is recommended only for those with normal cardiac function who have had prolonged hypertransfusion therapy to maintain hemoglobin levels at 10 g/dL and iron chelation therapy with deferoxamine blood pressure chart age 13 purchase 10 mg zebeta overnight delivery. In cases in which fetal growth is suboptimal arteria descendens genus order zebeta 5 mg, patients should have fetal surveillance blood pressure medication migraines order zebeta cheap online. Pregnant women with b-thalassemia minor and the associated asymptomatic anemia typically have favorable pregnancy outcomes. In the absence of documented iron deficiency anemia, replacement of iron beyond prophylactic doses is not indicated. Inherited Thrombophilias Inherited thrombophilias are a group of disorders characterized by a propensity for blood clotting. They are caused by defects in one or more of the clotting factors and often result in potentially dangerous thrombosis. In addition to the association between thrombophilias and thrombosis, there may be an associa tion between inherited thrombophilias and adverse pregnancy outcomes, such as fetal loss, preeclampsia, fetal growth restriction, and placental abruption; however, a definitive causal link has not been established. It is useful only when results will affect management decisions, and is not useful in situations where treatment is indicated for other risk factors. Screening may be considered in patients 216 Guidelines for Perinatal Care with a personal history of venous thromboembolism that was associated with a nonrecurrent risk factor (eg, fractures, surgery, and prolonged immobilization) or who have a first-degree relative with a history of high-risk thrombophilia or venous thromboembolism before age 50 years in the absence of other risk fac tors. Testing for inherited thrombophilias in women who have experienced a recur rence of fetal loss, placental abruption, previous intrauterine growth restriction, or previous preeclampsia is not recommended. Whenever possible, laboratory testing should be performed remote (after 6 weeks) from the thrombotic event while the patient is neither pregnant nor taking anticoagulation nor hormonal therapy. Management the decision to not use pharmacologic therapy or to treat with thrombopro phylaxis or full anticoagulation is influenced by the venous thromboembolism history, severity of inherited thrombophilia, and additional risk factors. All patients with inherited thrombophilias should undergo individualized risk assessment, which may modify management decisions. As the rate of obesity increases, the number of obese women of childbearing age considering bariatric surgery also increases, which results in questions about pregnancy after these types of surgeries. It is important for obstetric care providers to counsel obese patients with specific information concerning the maternal and fetal risks of obesity in pregnancy and to address prenatal and peripartum care considerations that may be especially relevant for obese patients, including those who have undergone bariatric surgery. Obesity During pregnancy, obese women are at increased risk of several adverse perina tal outcomes, including anesthetic, perioperative, and other maternal and fetal complications. Compared with nonobese women, obese patients are at high risk of preeclampsia; gestational diabetes; preterm birth; cesarean delivery; and Obstetric and Medical Complications 217 operative and postoperative complications, including prolonged operating times and increased rates of excessive blood loss, wound infection, thromboembo lism, and endometritis. Obese women are less likely to have a successful vaginal delivery than nonobese patients, and the success rate of attempted vaginal birth after cesarean delivery is very low in extremely obese women. Maternal obesity can have deleterious effects on the fetus, including increased risks of congenital anomalies, growth abnormalities, miscarriage, and stillbirth. The most common types of obesity-associated birth defects are related to the neural tube, cardiac systems, and facial clefting, even after controlling for the diabetes. In addi tion, increased body mass impairs visualization of ultrasound images and can compromise prenatal diagnosis of fetal anomalies. Maternal obesity also may be associated with an increase risk of subsequent childhood obesity. Nutrition consultation should be offered to all obese women and they should be encouraged to follow an exercise program. This consulta tion should continue postpartum and before attempting another pregnancy. Consideration should be given to screening for gestational diabetes upon presentation or during the first trimester and repeating it later in pregnancy if the initial screening result is negative. Because these patients are at increased risk of emergent cesarean delivery and anesthetic complications, anesthesiology consultation before delivery is encouraged. Because of the increased likelihood of complicated and emergent cesarean delivery, extremely obese women may require specific resources, such as additional blood products, a large operating table, and extra personnel in the delivery room. Particular attention to the type and placement of the surgical incision is needed (ie, placing the incision above the pannicu lus adiposus. The decision to perform a primary cesarean delivery for obese women should be based on standard maternal and fetal indications.