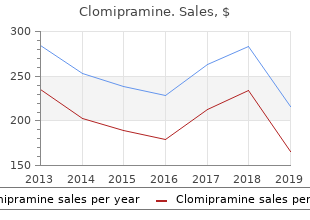
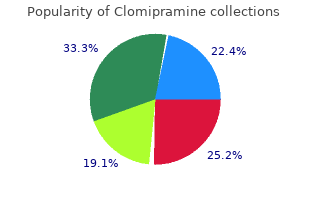
Clomipramine
"Best purchase for clomipramine, depression guidelines 2015".
By: S. Abbas, M.A., M.D., M.P.H.
Professor, University of Rochester School of Medicine and Dentistry
Throat and nasopharyngeal cultures are not recommended depression symptoms lethargy discount clomipramine 50mg with mastercard, because these cultures are of no value in deciding who should receive chemoprophylaxis organic mood disorder icd 9 buy generic clomipramine line. Chemoprophylaxis is warranted for people who have been exposed directly to depression reddit order cheap clomipramine online a patient�s oral secretions through close social contact, such as kissing or sharing of tooth brushes or eating utensils, as well as for child care and preschool contacts during the 7 days before onset of disease in the index case. People who frequently slept in the same dwelling as the infected person within this period also should receive chemoprophylaxis. For airline travel lasting more than 8 hours, passengers who are seated directly next to an infected person should receive prophylaxis. Chemoprophylaxis ideally should be initiated within 24 hours after the index patient is identifed; prophylaxis given more than 2 weeks after exposure has little value. Rifampin, ceftriaxone, ciprofoxacin, and azithromycin are appropriate drugs for chemoprophylaxis in adults, but neither rifampin nor ciprofoxacin are recommended for pregnant women. Recommended Chemoprophylaxis Regimens for High-Risk Contacts and People With Invasive Meningococcal Disease Age of Infants, Children, and Effcacy, Adults Dose Duration % Cautions Rifampina <1 mo 5 mg/kg, orally, 2 days every 12 h 1 mo 10 mg/kg (maxi 2 days 90�95 Can interfere with effcacy of oral mum 600 mg), contraceptives and some seizure orally, every and anticoagulant medications; 12 h can stain soft contact lenses Ceftriaxone <15 y 125 mg, intra Single 90�95 To decrease pain at injection site, muscularly dose dilute with 1% lidocaine 15 y 250 mg, intra Single 90�95 To decrease pain at injection site, muscularly dose dilute with 1% lidocaine Ciprofoxacina,b 1 mo 20 mg/kg (maxi Single 90�95 Not recommended routinely for mum 500 mg), dose people younger than 18 years of orally age; use may be justifed after as sessment of risks and benefts for the individual patient Azithromycin 10 mg/kg (maxi Single 90 Not recommended routinely; mum 500 mg) dose equivalent to rifampin for eradication of Neisseria meningitidis from naso pharynx in one study a Not recommended for use in pregnant women. Emergence of fuoroquinolone-resistant Neisseria meningitidis�Minnesota and North Dakota, 2007�2008. If antimicrobial agents other than ceftriax one or cefotaxime (both of which will eradicate nasopharyngeal carriage) are used for treatment of invasive meningococcal disease, the child should receive chemoprophylaxis before hospital discharge to eradicate nasopharyngeal carriage of N meningitidis. Ciprofoxacin, administered to adults in a single oral dose, also is effective in eradi cating meningococcal carriage (see Table 3. In areas of the United States where ciprofoxacin-resistant strains of N meningitidis have been detected, ciprofoxacin should not be used for chemoprophylaxis. Use of azithromycin as a single oral dose has been 1 shown to be effective for eradication of nasopharyngeal carriage and can be used where ciprofoxacin resistance has been detected. Emergence of fuoroquinolone-resistant Neisseria meningitidis� Minnesota and North Dakota, 2007�2008. Because secondary cases can occur sev eral weeks or more after onset of disease in the index case, meningococcal vaccine is an adjunct to chemoprophylaxis when an outbreak is caused by a serogroup prevented by a meningococcal vaccine. For control of meningococcal outbreaks caused by vaccine preventable serogroups (A, C, Y, and W-135), the preferred vaccine in adults and children 2 years of age and older is a meningococcal conjugate vaccine (see Table 3. Three meningococcal vaccines are licensed in the United States for use in children and adults against serotypes A, C, Y, and W-135. Both meningococcal conjugate vaccines are administered intramuscularly as a single 0. Routine childhood immunization with meningococcal conjugate vaccines is not recommended for children 9 months through 10 years of age, because the infection rate is low in this age group; the immune response is less robust than in older children, adolescents, and adults; and duration of immunity is unknown. However, a 1 meningococcal conjugate vaccine is recommended for children and adolescents who are in high-risk groups as a 2-dose series at 9 months through 55 years of age (Table 3. A booster dose at 16 years of age, is recommended for adolescents immunized at 11 through 12 years of age. Adolescents who receive the frst dose at 13 through 15 years of age, should receive a 1-time booster dose at 16 through 18 years of age. People at increased risk include: Children 9 months of age and older, including adults who have a persistent comple ment component defciency (C5�C9, properdin, factor H, or factor D). Children 2 through 10 years of age who travel to or reside in countries in which meningococcal disease is hyperendemic or epi demic should receive 1 dose. Children who remain at increased risk should receive a booster dose 3 years later if the primary dose was given from 9 months through 6 years of age and 5 years after the last dose if the previous dose was given at 7 years of age or older. Meningococcal immunization recommendations should not be altered because of pregnancy if a woman is at increased risk of meningococcal disease. All confrmed, presumptive, and probable cases of invasive meningococ cal disease must be reported to the appropriate health department (see Table 3. Timely reporting can facilitate early recognition of outbreaks and serogrouping of isolates so that appropriate prevention recommendations can be implemented rapidly. When a case of invasive meningococcal disease is detected, the physician should provide accurate and timely information about meningo coccal disease and the risk of transmission to families and contacts of the infected person, provide or arrange for prophylaxis, and contact the local public health department. Some experts recommend that patients with invasive meningococcal disease be evaluated for a terminal complement defciency. Public health questions, such as whether a mass immunization program is needed, should be referred to the local health department. In appropriate situations, early provision of infor mation in collaboration with the local health department to schools or other groups at increased risk and to the media may help minimize public anxiety and unrealistic or inap propriate demands for intervention.
Bulking agents anxiety 1st trimester generic clomipramine 50 mg visa, anti syndrome-diarrhea: effects on bowel frequency and intes spasmodics and antidepressants for the treatment of irrit tinal function mood disorder nos 29690 discount clomipramine 50mg otc. Effect of bre depression defined by dsm iv buy clomipramine 25mg, antispas able bowel syndrome and chronic idiopathic constipation. Benecial effects of sensation after lactose ingestion in a population with lac oral tilactase on patients with hypolactasia. Am J cebo effect: randomised controlled trial in patients with ir Gastroenterol 2013;108:707�17. The irritable bowel syn short chain carbohydrates alters the pattern of gas produc drome: review and a graduated multicomponent treatment tion and genesis of symptoms in irritable bowel syndrome. Personal view: food for thought� syndrome: long-term prognosis and the physician-patient western lifestyle and susceptibility to Crohn�s disease. Physical activity im Intervention on Irritable Bowel Syndrome: A Systematic proves symptoms in irritable bowel syndrome: a random Review. Irritable bowel syn abdominal symptoms in patients with irritable bowel drome in primary care: the patients� and doctors� views on syndrome: randomized placebo-controlled evidence. Food-related reduces symptoms of irritable bowel syndrome as well as gastrointestinal symptoms in the irritable bowel syndrome. British Dietetic intolerance in subjects with irritable bowel syndrome� Association evidence-based guidelines for the dietary Irritable bowel syndrome and diet | 19 management of irritable bowel syndrome in adults. The effect of a lactose ponent of food avour turmeric, reduces mucosal injury in restricted diet in patients with a positive lactose tolerance trinitrobenzene sulphonic acid-induced colitis. Br J test, earlier diagnosed as irritable bowel syndrome: a 5-year Pharmacol 2003;139:209�18. Sucrase-isomaltase and ameliorates trinitrobenzene sulfonic acid-induced col deciency. J Pediatr presses p38 mitogen-activated protein kinase activation, re 1973;83:721�7. Am J Physiol matory gene expression by inhibiting inhibitory factor Gastrointest Liver Physiol 2008;294:G217�25. Curcumin maintenance gastrointestinal symptoms in subjects without celiac dis therapy for ulcerative colitis: randomized, multicenter, ease: a double-blind randomized placebo-controlled trial. Curcumin in Combination gluten in patients with self-reported non-celiac gluten sen With Mesalamine Induces Remission in Patients With Mild sitivity after dietary reduction of fermentable, poorly ab to-Moderate Ulcerative Colitis in a Randomized Controlled sorbed, short-chain carbohydrates. Curcumin, a compo may improve irritable bowel syndrome symptomology in nent of turmeric: from farm to pharmacy. Ayurveda ism(s) for relaxant effects of Foeniculum vulgare on guinea and traditional Chinese medicine: a comparative overview. Both conditions are sacral root neurostimulation, surgery) are discussed, and practical included among the functional bowel disorders, and have a signifcant recommendations are made regarding each of them. Abdominal syndrome subtype, where constipation represents the predominant discomfort. Clinical complaint, in association with recurrent abdominal pain, bloating, practice guideline. Constipation is characterized by diffculties with or low frequency of bowel movements, often accompanied by straining during defecation or a feeling of incomplete evacuation. Why are irritable bowel syndrome with difference being the presence or absence of pain, albeit not in an constipation and functional constipation in the adult �all or nothing� manner. Furthermore, all the available cal changes that may be shown by routine diagnostic tech niques. Sociedad Espanola de Patologia Digestiva (Spanish Society of Digestive bowel syndrome with constipation and functional constipation in the adult. Doubtless, both conditions share myalgia or interstitial cystitis) is very common (12,13). Insuffcient criteria for irritable bowel syndrome *Criteria fulflled for the last 3 months with sympton onset at least 6 months before diagnostic 4. What is the clinical, social, and fnancial stool passage includes straining, a sense of incomplete signifcance of irritable bowel syndrome with evacuation, hard/lumpy stools, prolonged time to pass constipation and functional constipation Data obtained from Europe, specifcally from Spain, also show an increase in both direct and indirect 5. It surveys the intensity of 5 different items along 10 days: abdominal pain, disten sion, stool frequency, stool consistency, and interference with daily activities. Each item is scored on 0-to-100 visual analog scale, and all 5 scores are then added up.
Meticulous labeling mood disorder screening tool safe clomipramine 50mg, storage tropical depression definition wikipedia generic 10mg clomipramine amex, and verifcation of recipient identity before providing human milk should be practiced by child care providers depression definition finance best clomipramine 25mg. School Health Clustering of children together in a school setting provides opportunities for transmission of infectious diseases. Determining the likelihood that infection in one or more children will pose a risk for schoolmates depends on an understanding of several factors: (1) the mechanism by which the organism causing infection is spread; (2) the ease with which the organism is spread (contagion); and (3) the likelihood that classmates are immune because of immunization or previous infection. Decisions to intervene to prevent spread of infection within a school should be made through collaboration among school offcials, local public health offcials, and health care professionals, considering the availability and effectiveness of specifc methods of prevention and risk of serious complications from infection. Generic methods for control and prevention of spread of infection in the school setting include the following: � For vaccine-preventable diseases, documentation of the immunization status of enrolled children should be reviewed. Although specifc laws vary by state, most states require proof of protection against poliomyelitis, tetanus, pertus sis, diphtheria, measles, mumps, rubella, and varicella. In 2007, the Centers for Disease Control and Prevention recommended that all states require that children entering elementary school have received 2 doses of varicella vaccine or have other evidence of immunity to varicella. Physicians involved with school health should be aware of current public health guidelines to prevent and control infectious diseases. In all circumstances requiring inter vention to prevent spread of infection within the school setting, the privacy of children who are infected should be protected. Diseases Preventable by Routine Childhood Immunization Children and adolescents immunized according to the recommended childhood and adolescent immunization schedule (see Fig 1. Measles and varicella vaccines have been demonstrated to provide protection in some susceptible people if administered within 72 hours after exposure. Measles or varicella immunization should be recommended immediately for all nonimmune people during a measles or varicella outbreak, respectively, except for people with a contraindication to immunization. Many people without evidence of immunity may not yet have been exposed; therefore, vaccinating at any stage of an outbreak can prevent disease. Students immunized for measles or varicella for the frst time under these circumstances should be allowed to return to school after immunization. People who are immunocompromised, are older than 40 years of age, or have liver disease should receive Immune Globulin (see Hepatitis A, p 361). Update: Prevention of hepatitis A after exposure to hepatitis A virus and in international travelers. Respiratory tract viruses, however, are associated with exacerba tions of reactive airway disease and an increase in the incidence of otitis media and can cause signifcant complications for children with chronic respiratory tract disease, such as cystic fbrosis, or for children who are immunocompromised. Infection control prin ciples of respiratory etiquette�hand hygiene and covering mouth and nose with tissue when coughing or sneezing (if no tissue is available, use the upper shoulder or elbow area rather than hands)�should be taught and implemented in schools. Infuenza virus infection is a common cause of febrile respiratory tract disease and school absenteeism. Annual infuenza immunization should be administered to children and adults 6 months of age and older (see Infuenza Vaccine, p 445). Mycoplasma pneumoniae causes upper and lower respiratory tract infection in school aged children, and outbreaks of M pneumoniae infection occur in communities and schools. The nonspecifc symptoms and signs associated with this organism make distinguishing M pneumoniae infection from other causes of respiratory tract illness diffcult. Antimicrobial therapy does not necessarily eradicate the organism or prevent spread. Thus, intervention to prevent secondary infection in the school setting is diffcult. Mycoplasma outbreaks in schools should be reported to the local health department. Symptomatic contacts of students with pharyngitis attributable to group A streptococ cal infection should be evaluated and treated if streptococcal infection is demonstrated. Infected students may return to school 24 hours after initiation of antimicrobial therapy. Students awaiting results of culture or antigen-detection tests who are not receiving anti microbial therapy may attend school during the culture incubation period unless there is an associated fever or the infection involves a child with poor hygiene and poor control of secretions. Bacterial meningitis in school-aged children may be caused by Neisseria meningitidis. Infected people are not considered contagious after 24 hours of appropriate antimicrobial therapy. After discharge from the hospital, they pose no risk to classmates and may return to school. Prophylactic antimicrobial therapy is not recommended for school contacts in most circumstances.
Molecules classically regarded as (which some do) depression symptoms quotes cheap 75 mg clomipramine with mastercard, this descriptor should not be taken prebiotics include human milk oligosaccharides anxiety pain buy clomipramine no prescription, inulin bipolar depression lingers cheap 25 mg clomipramine mastercard, to imply probiotic activity. Probiotic in food or supplement without a health the concept of selectivity has been challenged. Bindels 27 claim et al proposed an alternative denition of a prebiotic as �a nondigestible compound that, through its metabo Such products state that they �contain probiotics. In support of the latter, they draw attention to the the absence of acceptable evidence of a health 33 demonstration of potentially benecial effects of pre benet. Probiotic in food or supplement with a specic also proposed that noncarbohydrates may act as prebiotics health claim and added the following candidate prebiotics to the usual list: �resistant starch, pectin, arabinoxylan, whole grains, this category requires that the product has demon various dietary bers, and noncarbohydrates that exert strated convincing evidence of a specic health claim January 2019 Prebiotics and Probiotics in Digestive Health 335 such as �reinforces the body�s natural defenses. The intent is to health claim: amplify the benets of the probiotic as well as stimulate a. Characterization of the strain or each of the the growth of indigenous benecial microbes. Identication of the health relationship that is Implications considered as a benecial physiological effect to the target population (ie, the general population the tersely worded legalize of the documents which or a dened part of it) typify the seemingly esoteric promulgations of the c. Demonstration of health effects in a normal various regulatory bodies do have signicant practical healthy population. In the United States, for example, where, in comparison with drugs, prebiotics, probiotics and syn Few probiotics have met these requirements. Probiotic drug confronted with products and formulations all claiming to be (or contain) probiotics whose range seems to be Here the probiotic is used to treat or prevent a spe limited only by the imagination of the manufacturer. In the United States, and elsewhere, this Claims deftly skirt around preventing or treating disease is now categorized as a drug (dened as an article by the use of vague terms such as �immune boosting� or intended for use in the diagnosis, cure, mitigation, �restoring digestive balance� yet are seldom supported treatment, or prevention of disease) and must satisfy all by any clinical data. How is the hapless consumer to the regulatory requirements to be approved as such. It seems inevitable drug, it is regulated in the United States under the Di that regulatory oversight must increase. This will pose require approval by the Food and Drug Administration challenges for potential investigators; specically, who before being marketed but, according to Dietary Sup will fund the trials which will be required to satisfy the plement Health and Education Act of 1994, must provide new demands of regulatory authorities�requirements 41,42 evidence of safety and follow Current Good that are already beginning to emerge in Europe If it Manufacturing Practice requirements for dietary sup is decided that a given probiotic product is to be regarded plements. Serious adverse events must be reported to as a food, prot margins will be slim and the target 36 population will, by denition, be the healthy population. The regulatory approach in other jurisdictions varies considerably from Such trials will by virtue of their endpoints require very treating nonfood probiotics as drugs or biological agents large numbers of participants and be very expensive. In others, there is Within the food category one acceptable endpoint would 37 be the demonstration of a reduction in risk for a given minimal oversight. The current denition of a probiotic has further entity in the general population. Two issues deserve special emphasis: the biomarker of risk, of which there are few (eg, cholesterol focus on �live� organisms and the insistence on for heart disease), not a biomarker of early disease (which conferring �a health benet on the host. In other words, it may be cheaper to study infective effects, this strategy has not, as yet, been probiotics as drugs for narrow indications within the explored or validated in humans. It seems improbable pharmaceutical sector (paradoxically lower costs and thateffectsofprobioticsinhumanswillbeconned to higher margins on licensable product) unless new mi live organisms so this aspect of the denition will ulti crobial biomarkers of risk emerge. The term pharmabiotic has been proposed Practical Considerations to encompass all biological active moieties derived from the microbiota. Second, it is obvious from the latter part of Quality Control the denition that clinical claims in humans, be they in the augmentation of health or in the treatment of disease, Any prebiotic that is recommended for use in humans must be supported by credible clinical trial data. While this painstaking approach to pro 51�53 effects of gastric acid, bile, and digestive enzymes so that biotic discovery has been adopted by investigators it arrives at its proposed site of action (usually the colon) and reputable manufacturers, many products on the intact. Dose ranging studies should be performed to market have not been subjected to even the most basic ensure that an effective dose is delivered without causing aspects of quality control. Needless to say, any and all health biotic and prebiotic usage have been given scant atten claims should be supported by clinical evidence and tion, such as optimal dose and ideal formulation. Strain every effort should be made to establish a cause-and selection is critical. While certain bacterial properties effect relationship between the administration of the may be common to some or all members of a given prebiotic, changes in microbial populations and their species, others, including those that may well be relevant metabolism and the health benet.
Having extended the variant by a 15 cm sulphur block resulted in the reasonable decrease of the epithermal flux by 43% but the fast neutron dose ratio decreased only by 32% bipolar depression symptoms in women cheap clomipramine 50mg on-line. The present heterogeneous design consists of the alternating blocks of Al and AlF3 depression symptoms muscle pain proven clomipramine 10mg, totally 40 cm of Al plus 25 cm of AlF3 depression symptoms wiki generic 50mg clomipramine overnight delivery. The safety and utility of the facility were improved due to the Safety Observation System. By November 1995, just before the remodelling, sixty-one clinical trials were carried out for about six years [6]. Moreover, the following problems of the old facility had been pointed out; (i) difficulty of the handling for the routine maintenance and checkup, and for the irregular damage, and (ii) risk of the leakage of the cooling light water for the heavy water tank, because of its structure that the heavy water tank was settled on the reactor tank with an 0-ring of about 2 m diameter by thirty-six stainless-steel bolts and the primary cooling water flew through a narrow channel between the both tanks. In regard to these matters, the necessity of the fundamental reconstruction of the whole facility became remarkably recognised, from the viewpoint of the safety and stability of the facility and its usage. The design studies were performed mainly by simulation calculations using transport calculation codes for neutrons and gamma rays. The proprieties of the simulation calculation codes and the calculation processes were confirmed from the comparison between the measured data and calculation results for the old facility [8]. Improvement in safety for the facility From the standpoint of the improvement of the facility safety, the following subjects were carried out. In order to hold argon gas activated in the air gap, �Activated Argon Attenuation System� was installed. Exceptionally, the outer lead layer can be independently removed for the maintenance of the cadmium and boral filters, which were installed on the core-side of the outer lead layer. A design criterion of the Radiation Shielding System was that a total dose equivalent rate of neutrons and gamma rays was less than 100 m Sv/hr at the working area in the irradiation room. Moreover, in the viewpoint of the reduction of the working time in the irradiation room, the Remote Carrying System for a patient was 132 produced. A clinical collimator is settled on this system, then the positioning for the patient are possible outside of the irradiation room previously to a clinical irradiation. The numerical values are proper for a free-in-air condition with no irradiated sample at the normal irradiation position, which corresponds to the central point of the bismuth layer surface. The neutron energy regions for thermal, epi-thermal and fast neutrons are defined to be below 0. The ratio of the �11 2 incident gamma ray dose to thermal neutron fluence is less than 3 x 10 cGy/(n/cm). For the incident fast neutron dose, the incident ratio to thermal neutron fluence is less 2 than 1 x 10�11 cGy/(n/cm). For the incident gamma ray dose, the ratio is almost the same as that for the thermal neutron irradiation field. The ratios of the incident gamma ray dose and fast neutron dose to epi-thermal 2 0 2 neutron fluence are less than 3 x 10�~ cGy/(n/cm) and 1 x i0~� cGy/(nlcin), respectively. The epi-thermal neutron moderator, the neutron energy spectrum shifter, the thermal neutron filters and the bismuth layer were installed in order from the core side. As the heavy water tank was settled not connectedly with the reactor tank, it can be removed together with the polyethylene layer and the lead layer outside of the tank. The cooling water jackets of 1 cm thickness are attached both to the reactor tank and the heavy water tank. The inner lead layer of 10 cm thickness and the outer lead layer of 20 cm thickness were settled for the gamma ray shielding. This inner lead layer is an effective shielding against the gamma rays from the core side under the maintenance work. Between the inner and outer lead layers, a polyethylene layer is inserted as a supplementary shield against fast neutrons. The epi-thermal neutron moderator and the neutron energy spectrum shifter the installation position of the epi-thermal neutron moderator was restricted to be the inside of the heavy water tank adjacent to the reactor core. From the design study results on priority of the safety and stability, the moderator was decided to be 80%/20% in the mixing volume-ratio of aluminum and heavy water, 60 cm in diameter, and 66 cm in thickness. The periodic structure of 20 mm-thick aluminum plates and 5 mm-thick heavy water gaps was decided, on the expectation of the heat removal by natural-convection. That is because (1) we had much experience for the utilisation and handling of aluminum and heavy water at the old facility, and (2) these materials had been considered as a moderator in some plans for the epi thermal neutron irradiation field [9,10]. The spectrum shifter is comprised of three shifter tanks of almost 70 cm diameter, whose thickness are 10, 20 and 30 cm in order from the reactor core side.
Buy discount clomipramine line. What is MDD depression ? | Health News and FAQ.